
Introduction
Having gut-wrenching nightmares every night is no fun. In fact, it can get troublesome to the point of haunting. Coming across nightmares once in a while is often common for many of the population. However, it is an entirely different matter with extremely frequent nightmares. Nightmare sufferers, as a general term, point toward individuals whose quality of life nightmares greatly disturb1. In addition, with recent research, nightmares have actually become a worthwhile clinical concern.
The Part 1 post below detailed personal experience of a veteran polyphasic sleeper and improved nightmares. Therefore, this post will focus more on certain scientific aspects of sleep architecture in nightmare sufferers, including their napping habits. Ultimately, some other factors relevant to nightmare experiences and polyphasic sleep will also be on display. This would hopefully help to delve into polyphasic sleeping’s niches for nightmare sufferers and to what extent they can cope with their problems.
DISCLAIMER: Even though the healthcare and medical professionals have a severe lack of understanding on treating nightmares2, we do not give medical advice. Hence, readers should only consider the content of this post a possible pointer to dealing with nightmares. How effective the strategies are all depend on several interindividual factors.
Content
- Sleep Mechanics of Nightmare Sufferers
- Implications for Polyphasic Sleep
Sleep Mechanics of Nightmare Sufferers
General Assessments
Nightmare sufferers, by definition, suffer from nightmares. Now, does it mean having nightmares every night? Surprisingly, that does not have to be the case.
- According to International Classification of Sleep Disorders (2nd edition), recalling at least two nightmares or bad (dysphoric) dreams per week for 6 months is sufficient1. Note that, though, these nightmares did not cause participants to wake up at night.
- There is a general consensus on the existence of clinical impacts of nightmares on daily activities1.
- Alongside a high frequency of nightmares, sleep disorders, such as sleep paralysis, night terrors, insomnia and interrupted sleep are present4.
- Nightmare sufferers also usually have less slow spindle density, while much “faster” fast spindle activity3.
- Early childhood (0-6 years) adversities, such as neglect, separation, abuse can also reduce slow spindle density4. Furthermore, current psychopathic symptoms such as PTSD are often common in such cases4.
- In comparison with control group, nightmare-prone subjects experienced intensified daydreaming5. These instances were more bizarre, positive and caused elevated body sensations. However, the negative rating was not different between both groups.
- Per sleep quality, nightmare sufferers have somewhat higher NREM2 duration and higher sleep onset than healthy subjects6. It also takes them longer to actually fall asleep (or enter NREM2). Together with sleep spindle composition, these abnormalities constitute psychopathological sleep architecture. However, nightmare sufferers seem to have normal sleep duration.
Overall, these factors can culminate in suicidal ideation3, at least in more severe cases. It is also reasonable to expect that nightmare-prone individuals have more subpar sleep quality than usual.
Nightmare Dream Contents
With the extreme scarcity of nightmare sufferers in the polyphasic community, this section only analyzes research-based dream reports. As a result, the dream reports are mostly monophasic sleep, with an exception of some biphasic sleep practice.
- During diary dreams, nightmare participants showed higher sensitivity and higher rating of negative than positive dream elements7.
- Dysphoric dream distress has a negative correlation with frontal activation during negative picture viewing3. Overall, there is a much stronger reactivity toward dream images in nightmare group than control group.
- Dream reports of nightmare group were only slightly longer than control6.
Study 1
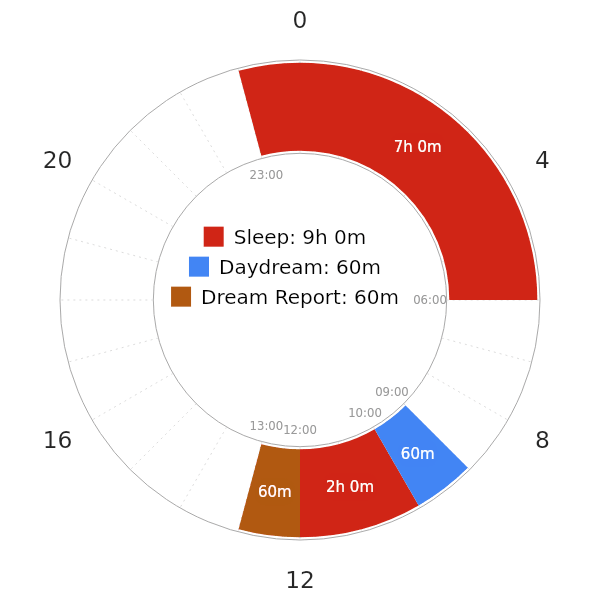
The short-term study below examines the napping experience in nightmare sufferers. Below are the findings5:
- Although nap dreams showed no differences in positive or negative contents, daydreams of nightmare group were much more positive and vivid than control.
- However, in this study, no participants slept through the 2-hour window. Instead, they were awakened after 10 minutes entering REM sleep. They also slept a normal duration at night, before arriving at the laboratory. Thus, this would constitute a non-reducing Siesta schedule with a minimum of~50 minutes of actual sleep in the nap.
- This setup was one of the very few experiments on napping behavior of nightmare sufferers.
- Contrary to the expectation of abundant negative dreams, the nightmare group did not definitively go through “painful” dreams. The study does offer some explanations:
- First, early-night dreams are more negative than late-night dreams. Specifically, dreams that occur near the highest propensity hours for REM sleep have different emotional content from early-night dreams. There was some prior scientific evidence that late-night dreams are less negative, as a result.
- Second, sleeping in the laboratory may have suppressed nightmares. It is then possible, that sleeping under supervision of sleep professionals helps alleviate anxiety.
Study 2
The non-reducing Siesta variant in this short-term study is similar to that in the first study. None of the subjects experienced nightmares every night before the study, either. Below are the highlights6:
- Nightmare subjects have peculiar emotional semantic associations.
- The “siesta” leads to restricted breadth of associations for primed negative cue-words.
- Likewise, REM naps lead to increased breadth of associations for primed positive cue-words.
- After one week, control group no longer showed altered semantic access for primed words.
- Nightmare sufferers retained their priming effect after the retest one week later.
Note that the priming effect describes cue-words that had been memorized prior to napping. The study also implies that the nightmare group appears to be more creative. This is due to their modified REM-sleep dependent emotional processes over time. It is also worth noting that “REM nap” is an umbrella term for any polyphasic naps that contain at least some REM sleep.
Abnormalities of REM Sleep & NREM Sleep
Although nightmares mostly occur during REM sleep5, we also know that any sleep stages can generate dreams. As such, REM sleep processes are not entirely independent from NREM sleep. In fact, comorbid pathologies in nightmare sufferers suggest that NREM sleep (sleep spindles) is affected as well9. This section will dive into the oddities in REM sleep of nightmare-prone individuals mostly. As usual, the mileage may vary, and there are some contradictory results.
- There are some changes in theta activity during REM sleep of nightmare sufferers1. Specifically, higher slow theta activity (2-5 Hz) was present during NREM and REM sleep. The differences, however, were most prominent during every REM sleep cycle except the first cycle.
- There was, regardless, not much change in REM sleep distribution and duration compared to control1. Still, frequent nightmare recallers often generate higher theta activity in a prefrontal-limbic circuit in all sleep-wake stages, especially during REM sleep. This circuit is often known for regulating influences on the processing of memory recall and emotion and guiding adaptive behavioral responses9.
- Most notably, a preliminary study demonstrated that with and without REM sleep deprivation conditions, nightmare recallers often have low need for REM sleep10.
- Even during recovery from sleep deprivation, these subjects displayed a reduced percentage of REM rebound. Furthermore, they did not seek treatment for nightmares at all.
- Similar to the previous study5, these subjects seem to normally cope with nightmares, although to which extent is unclear.
- An explanation for the low REM need is owing to the sleep-disrupting ability of nightmares. As mentioned earlier, nightmares are capable of decreasing sleep quality and preventing sleepers from getting vital sleep stages.
Implications for Polyphasic Sleep
As the Part 1 post about nightmares covered, nightmares are unpleasant and can be mentally troubling. Regular and uncommon nightmares have a strong association with adaptation to life stressors3, but frequent nightmares indicate low well-being1. Because the polyphasic community has not had many nightmare sufferers, the experience of two following veteran polyphasic sleepers may be interesting.
Polyphasic Sleep Experiences from People with Nightmares Every Night
- Both of these sleepers have been naturally Segmented sleepers. Hence, they have both been staying on a Dual Core lifestyle for several years. That includes a very flexible variant, DUCAMAYL with 1-2 naps alternating from day to day.
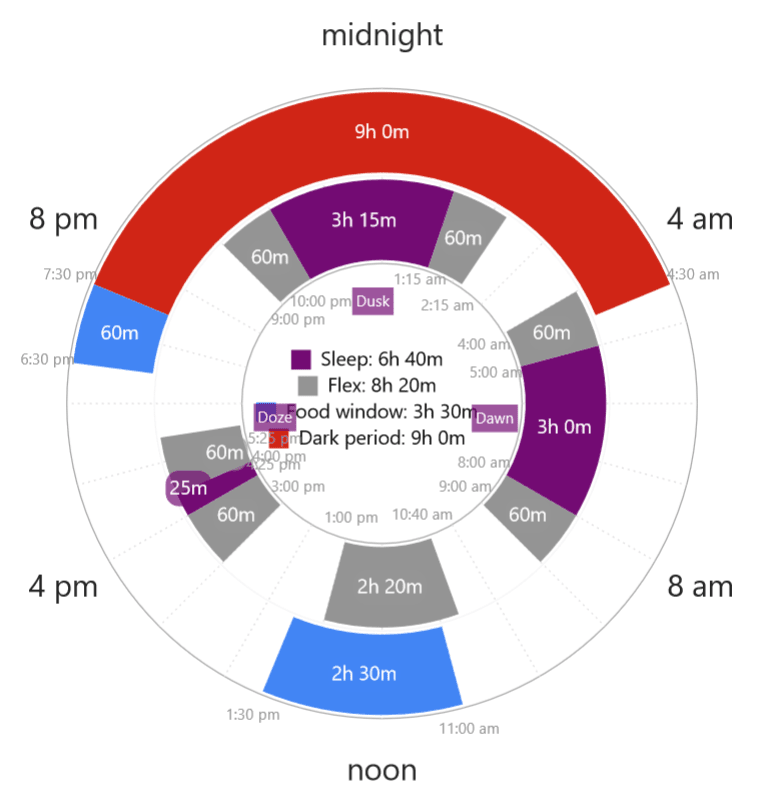
- This DUCAMAYL sleeper stated that his nightmares and sleep paralysis disturbed him in the middle of the night. He woke up, and had difficulty returning to sleep. Over time, he decided to wake up at night, stay up for some time before returning to sleep until morning. This Segmented habit greatly resembles the preindustrial sleep pattern that we have come to know!
- First, he structured his sleep times to be consistent.
- When his sleep quality improved, his mental symptoms during the day also alleviated.
- Overall, he ran into much fewer nightmares since then, and naturally adapted to a polyphasic pattern, with daytime naps.
- One sleeper has PTSD, and does experience bad dreams on her schedule. However, she has grown to embrace her Segmented and DC1 schedules over the years. Refer to her interview below from the Community YouTube channel.
- Both sleepers also did not reduce a lot of sleep from their personal monophasic baseline. This may be a very useful tool to sleep polyphasically without the long-enforced mentality that there has to be hefty sleep reduction.
Explanations
A viable explanation is using the circadian rhythm and sleep pressure concepts.
- There is much less REM sleep duration during the first core sleep, and much more during the second core. Using the reference from the aforementioned study, dreaming in the second core (during high REM-propensity hours, or REM peak) can lessen the intensity and/or appearance of nightmares. This observation is in line with the polyphasic sleepers’ dreaming experiences, with stable sleep timing.
- Having a stable sleep schedule with entrained sleep habits helps sustain sleep quality. This does not have to be a traditional monophasic schedule. In addition, nightmares that cause nocturnal awakenings may be the cue to starting a Segmented sleep schedule!
- A bonus is that polyphasic sleep can also reduce insomnia effects by increasing sleep quality within each sleep session. This factor is crucial in getting enough SWS and REM sleep each day.
Cautions
Although mostly hypothetical, the following explanations derive from healthy long-term polyphasic practice of some veterans. There are certain cautions against attempts to use polyphasic sleep to “treat” nightmares.
- A steep reduction in total sleep time likely will not solve the problems. This is because of the highly intense sleep deprivation symptoms that ensue during the adaptation process.
- Certain psychiatric disorders may aggravate with prolonged sleep deprivation. Examples include more mood swings and random outbursts. See Selective Sleep Deprivation Effects.
- If nightmares persist every night upon returning to monophasic sleep, think of a polyphasic schedule that can fit personal lifestyle in the long run.
With all these precautions, it is necessary to “experiment” with more basic and succeeded polyphasic schedules. Simply dividing sleep into two segments alone may yield much better results than expected.
Conclusion
In sum, it is possible to encounter nightmares every night. While the polyphasic community has rare samples, polyphasic sleeping does have a niche in coping with insomnia. Additionally, there are also anomalies during sleep of nightmare-prone individuals, as well as their REM sleep’s functions. However, nightmare’s mechanisms still remain ambiguous at large; it will require extensive testing and understanding of brain wave activities and internal sleep processes.
Meanwhile, polyphasic sleepers may further enhance understanding in their brave wave activity to detect any possible anomalies during sleep. For cases with nightmare sufferers, it is likely important to maintain consistent sleep habits; they can also probably use napping as a tool to cope with nightmares. More research is necessary to determine how much fragmentation of sleep is acceptable on a polyphasic regime, to not jeopardize REM sleep.
Main author: GeneralNguyen
Page last updated: 31 May 2021
Reference
- Marquis, Louis-Philippe, et al. “REM sleep theta changes in frequent nightmare recallers.” Sleep 40.9 (2017). [PubMed]
- J., T., M., N., M., von A., T., zcan, & R., P. (2014). Nightmares: Knowledge and attitudes in health care providers and nightmare sufferers. Journal of Public Health and Epidemiology, 6(7), 223–228. doi:10.5897/jphe2013.0565.
- Creamer, Jennifer L., et al. “Nightmares in United States military personnel with sleep disturbances.” Journal of Clinical Sleep Medicine 14.3 (2018): 419-426. [PubMed]
- Nielsen, Tore, et al. “Early childhood adversity associations with nightmare severity and sleep spindles.” Sleep medicine 56 (2019): 57-65. [PubMed]
- Carr, Michelle, et al. “Intensified daydreams and nap dreams in frequent nightmare sufferers.” Dreaming 26.2 (2016): 119.
- Carr, Michelle, et al. “Nightmare sufferers show atypical emotional semantic associations and prolonged REM sleep-dependent emotional priming.” Sleep medicine 20 (2016): 80-87. [PubMed]
- Picard-Deland, Claudia, et al. “Sleep spindle and psychopathology characteristics of frequent nightmare recallers.” Sleep medicine 50 (2018): 113-131. [PubMed]
- Carr, Michelle, et al. “Frontal brain activity and subjective arousal during emotional picture viewing in nightmare sufferers.” Frontiers in neuroscience 14 (2020): 1032. [PubMed]
- Kalin, Ned H. “Prefrontal Cortical and Limbic Circuit Alterations in Psychopathology.” (2019): 971-973. [PubMed]
- Nielsen, T. A., Paquette, T., Solomonova, E., Lara-Carrasco, J., Popova, A., & Levrier, K. (2010). REM sleep characteristics of nightmare sufferers before and after REM sleep deprivation. Sleep Medicine, 11(2), 172–179. doi:10.1016/j.sleep.2008.12.018. [PubMed]